

Today was wild. Not only did Saman and I shadow in the greatest department in the entire hospital yet again (urology), but we saw 4 surgeries in a row!
The first surgery we say was a kidney stone removal. We changed into our scrubs and met our surgeon we were shadowing in the operating room. The patient was already knocked out in supine position on the table, and the residents were painting the abdomen with povidone iodine (an antiseptic that appears orange).
We never actually caught our surgeon’s name, and so we decided to refer to him as “Super-Surgeon” after what we saw today (I’ll go into the details). Super-Surgeon told us that there are 3 ways to remove kidney stones in a patient: shock wave lithotripsy, laparoscopy, and something he referred to as “BNL”. BNL was invented in 1994 in Spain, and would be the procedure that we would be using today where the patient is put in supine and both a laparoscope and a catheter would be inserted so that all the stones could be retrieved (something called the “retrograde laparoscopic approach”). He told us that in the U.S., this procedure is performed in prone position but this is not as good because it is harder for the anesthesiologist to reach the patient’s airways. Contrast was inserted into the catheter and the physicians used a CT scan to see where the 3 cm right kidney stone was. The doctors used an endoscope and a tiny laser to break up the stone. It looked like a video game: the surgeon found the stone which looked like an asteroid and then aimed and shot at it until it broke into tiny pieces.

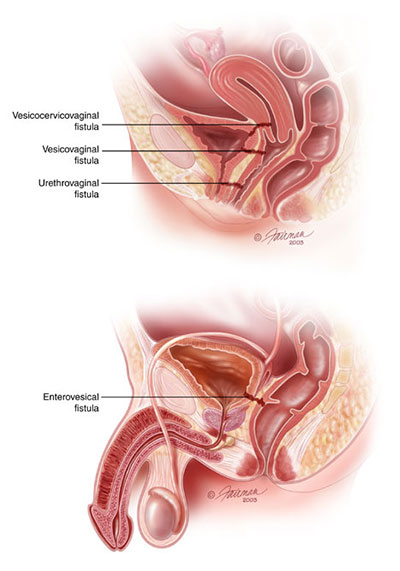
As our first surgery came to a close, Super-Surgeon told us to peek into OR 5 to see what they were up to in there. We walked in. It was dark, and everyone was huddled around the TV above the operating table wearing sunglasses. The first thing I thought was, why are they wearing sunglasses? Sarah the resident walked up to us and handed us sunglasses, and as soon as I put them on I realized why everyone was wearing them. They were 3D glasses and all the surgeons were observing the surgery in 3D! After the robot surgery on the first day, I thought the urology department couldn’t get any more advanced, but I was proven wrong. They were repairing a fistula (hole) that had developed between the large intestine and the bladder.
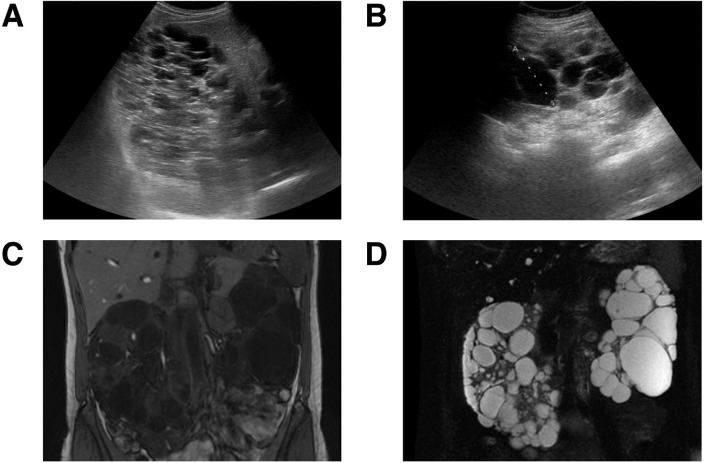
The third surgery was a patient that needed kidney stone removal from their transplanted kidney. The patient was relatively young with a genetic form of renal polycystosis: a disease where the kidneys develop non-cancerous cysts that cause the kidneys to lose function overtime. We were able to look at the patient’s kidneys on the CT scan: they were incredibly swollen and bumpy, I had never seen kidneys that looked so strange before! Super-Surgeon explained that a kidney stone removal from a transplanted kidney is more difficult than from a natural kidney because it is harder to find the entrance of the ureter into the bladder, and sometimes the ureter is narrowed. When the ureter is narrowed, there is a higher probability of infection, and in a patient with a compromised immune system this can be very dangerous. When Super-Surgeon entered the bladder and viewed the ureter through the endoscope, he realized it was too narrow to begin the stone removal process. He placed a stent in the ureter and informed us that he would check it in approximately 2 weeks and complete the full surgery.
Finally, we made it to the last and final surgery of the day. It was another kidney stone removal, but this patient had a congenital (from birth) disorder called medullary sponge kidney. In medullary sponge kidney, the collecting tubules are dilated, promoting the development of kidney stones. However, the stones are not able to leave the kidneys because they are stuck behind a mucous membrane. Super-Surgeon told us that the main goal of this surgery would be to break the mucus membrane, allowing the kidneys to “give birth” (his words, not mine) to the stones. He would pulverize the bigger stones into dust so that the patient could easily pass the stones by themselves.
By the time we finished observing the last surgery, we were exhausted. We got lunch and headed back to the dorms, and later that night we all went out for dinner together and got a nice group picture in front of the Iglesia de San Pablo, seen below:

I know this post is a little late, but I will be sure to catch up and continue to update you all on the crazy things (in and out of the hospital) I see in Spain! Ciao!
