Our group activity this week was wine tasting at a local winery called Enima located just outside the city. We started with a tour of the winery, we got to see the vineyards with hundreds of different kinds of grape as well as the factory where they aged, bottled, and packaged the wines.
The vineyards with all the grapes (most were white grapes for white wines).
We got to sit down and taste two different kinds of olive oil, served in small rounded glasses that we had to warm with our hands. Both oils tasted earthy and delicious, and the second one had a slight kick to it after you swallowed. Then we tasted the wines. Our tour guide told us that Spaniards (as well as most Europeans) only drink white wines in the summer, and red wines in the winter. She made us observe the wine and smell it before we actually did any tasting. I’m no wine expert (and they all kind of smelled the same to me) but I felt pretty fancy trying to guess the flavors that were in each glass. We tried two of their most popular white wines. The first one was very light and dry, and the second one was amber in color and sweet like a cider. I liked the second one much more than the first.
About to taste some wine!The placement says: “There are things that only pass with wine”
After we
finished at the winery, we went to El Castillo de la Mota (English: “The Castle of the Hill”) in Medina del Campo. El Castillo
was not just any castle, it was a medieval fortress built in 1080, complete
with a really creepy dungeon and a spiral staircase leading up to a large
watchtower. Our tour guide told us that since this was a fortress and not a
traditional castle, no queens or kings lived there. It was more of a functional
military center used to protect the city below the hill. However, she told us a
sad story about the queen Juana la Loca (“Joanna the Mad”) who was imprisoned in the fortress
for much of her life because she suffered from various “mental illnesses”. Apparently, Juana’s husband was famous for sleeping
with other women, and she spent much of her time trying to escape the castle in
order to catch him in the act.
Lili, me, Saman, and De’Ryonne at the castle.
After
exploring the castle, we went to get lunch at a cute little restaurant in the
surrounding city. I had a tuna-salad dish that was very delicious. Ciao!
Today we were back with the first Nacho, the bald one we had on Monday. I finally asked Carla (our site manager) why Nacho is such a common name in Spain even though its a type of cheese, and she told me its the nickname for “Ignacio”.
Our first surgery was a fun one because the bone saw came out. Our patient was a female in her 80s with a hip fracture located on the neck of the femur. Dr. “Ignacio” told us that when a fracture occurs there, no blood supply to the head of the femur is received, causing the tissue to become necrotic. He would need to put in a new, artificial head and neck of the femur. If the trochanter was the part that was fractured, he could simply put in a nail to fix it.
Out came the electric bone saw. Dr. Nacho was teaching a resident how to perform the surgery. She was a small girl about my size and I kept wondering how she was going to pull this off: all the other orthopedic surgeons I had seen thus far were large, muscular men. However, she ended up surprising me. Blood was spattering everyone’s scrubs, face, and glasses but the resident kept going with incredible accuracy and steady hands. I must have been making an uncomfortable face because the anesthesiologist walked up to me and said: “I don’t like the sound of it either. You get used to it though.”
The resident chopped off the head and neck of the bone and then hammered the stake deep within the femur. The socket prosthetic slipped right into the acetabulum of the pelvis, and she sewed up the patient like it was no big deal.
Our second surgery was another hip replacement, but this one was for a non-ambulatory female in her 90s. This time, Dr. Nacho was leading, and he told us that he traditionally prefers the posterolateral approach to hip replacements: entering the joint from the backside verses the lateral approach (side) or anterolateral approach (front).
The posterolateral approach to a hip replacement. Dr. Nacho told us there’s really no difference between the different types of approaches, its all about the surgeon’s preference and what they were taught.
Dr. Nacho did the surgery within 2 hours without any complications, while still joking around with the other surgeons and spraying them with sterilizing water. I realized that I would miss the orthopedics department. All the surgeons I had met were fun people, and I mean that in the most sincere way. They made sawing bones fun.
The dreaded European heat wave finally came upon us.
No matter how high we turned our fans, opened our windows, or fanned ourselves
with our notebooks, it was sweltering: 100 degrees Fahrenheit, 38 degrees
Celcius, and a whole lotta degrees humid.
De’Ryonne wasn’t feeling well because of the intense
heat so I went to the hospital alone on Wednesday. I would be shadowing Dr.
Nacho, however it wasn’t the Dr. Nacho I remembered. This Dr. Nacho was young:
he looked like he was about 30 years old, and he was tall with dark hair and a 15
o’clock shadow (in Spain time). He was very serious and spoke very softly so I
had to lean in to listen to him, but he spoke very fluent English which was
great.
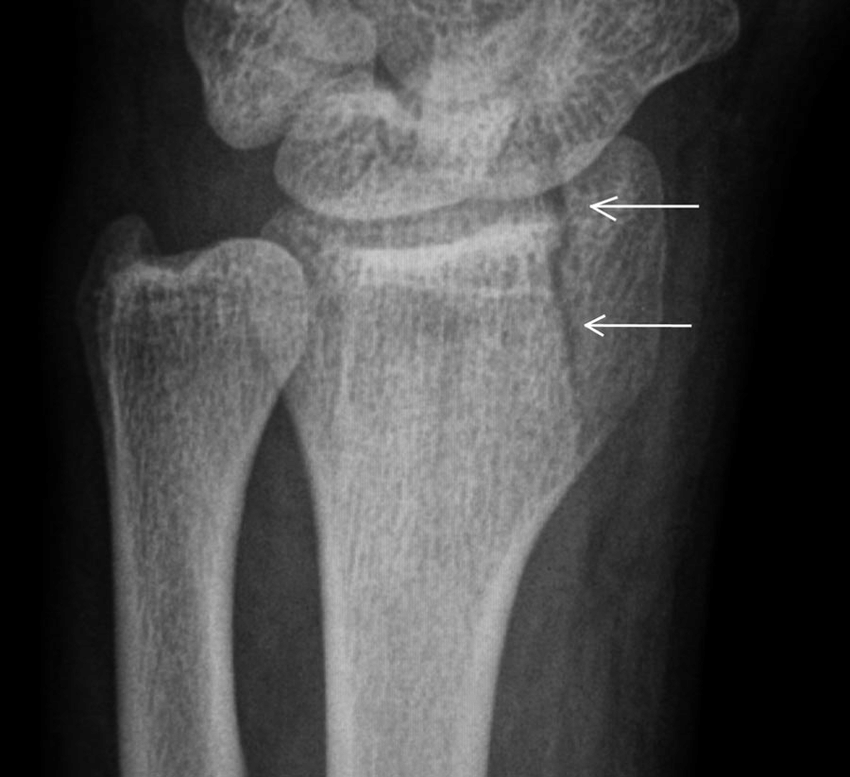
We walked down to the OR to start our first surgery: a
knee repair. The patient was a young female in her 40s who suffered from a fracture
in the distal femur. Dr. Nacho 2.0 told me that there are two types of repair
for this type of injury. The first one is putting in a nail. The second is a
plate. In this surgery, he would be choosing the second option.
Distal fracture of the femur as shown using an x-ray.
He took a CT scan of the knee and entered on the
lateral left knee with the scalpel. After putting in the plate and 8 screws,
all while the patient was snoring very loudly, he did two layers of a
non-continuous cruciate suture to sew up the skin. Finally, he stapled the skin
closed and put a large bandage over the area.
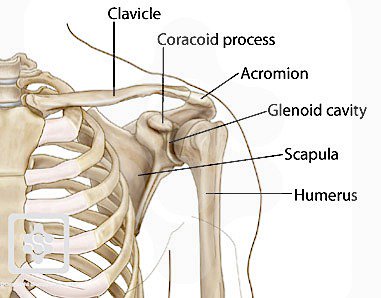
The second surgery was a distal clavicular fracture.
Dr. Nacho 2.0 told me he would be repairing it using a plate with a tiny rope
attached that would tie to the coracoid process to stabilize the clavicle. Dr.
Nacho said he had never used this tiny rope device before, but he was ready to
try it out.
The bones of the shoulder showing the coracoid process where the rope attached.
The patient was put under complete anesthesia because it
is impossible to give local anesthesia to the clavicular area (according to Dr.
Nacho 2.0). He used a cauterizer to cut the skin open and then used a hand-held
screwdriver to drill holes into the clavicle where the plate attached. The
surgery was incredibly fast for being his first time, but he kept having to
take CT scans to make sure everything was lined up inside. At the end, he asked
me if I had any questions, and then we said a formal goodbye and I scurried
home.
Orthopedics seems a little repetitive with the things they repair, but each case is completely different from the next. Plus, each specialty probably seems repetitive to people like me who only observe for 4 days at a time. It makes me want to learn their entire scope of practice: What other bones can they repair? What’s the strangest case they’ve had? What kinds of complications come with bone repair? I’ll let you know after the next blog post! Ciao!
On Tuesday, De’Ryonne and I were with a different surgeon,
a man named Dr. Jose Cantores. He was a middle-aged man with dark hair who
spoke English very well. Our first surgery was a man in his 30s with a right knee
fracture and a medial ligament tear. When I asked Dr. Cantores how this man got
his injuries, all he said was “he jumped off of something”.
Dr. Cantores waited about 10 minutes for the epidural
to kick in and then grabbed the cauterizing knife and went straight for the
lateral knee. He opened the joint capsule and cut through the lateral meniscus,
where he found the broken fragment from the fibula. Using the CT scan to
position the drill, he inserted a plate and attached it to the bone with pins. There
was a little extra space between the broken fragment and the fibula, which he
filled with crumbles of bone donated from a human cadaver. When I asked about
it, Dr. Cantores told us that the patient’s body would eventually replace the
donated bone crumbles, but it would work as a structural substitute until the
bone started to grow back. After the plate was positioned, he removed all the
pins and placed 6 screws in instead to stabilize. He sutured the muscle back
into place, and stapled the skin. Dr. Cantores told us that the patient would
recover in about 2 weeks, but would need to be non-weight bearing during recovery.
We quickly moved on to our second surgery: a trauma
case where a man had a hip fracture on his left leg and a broken ankle on his
right leg. The patient was pretty beaten up from head to toe, it looked as if
he had fallen down an extensive staircase and scraped and bruised his head,
face, chest, knees, and feet. His ankle was purple and swollen, and after they
removed his clothes you could tell that his hip was slightly swollen as well. The
nurses hung up a giant sheet of clear plastic in front of the surgeon and the hip
so that the patient was on one side, and the surgeon was on the other. There
was a tiny hole where Dr. Cantores could access the hip, but I had never seen
something like this before. Dr. Cantores called it the “Vertical System”, a way
to keep things completely sterile but also allow the surgeon to view the patient.
He told us: “Prevention is the only way to avoid infection”, and that the Rio
Hortega Hospital prides itself on being completely microbe-free.
The hip fracture was located right under the trochanter of the femur, so Dr. Cantores hammered in a large nail right through the fracture and into the center of the femur bone. A screw was placed horizontally towards the head of the femur to hold the nail in place. An additional smaller pin was placed further down the femur to stabilize the nail. The wounds were closed with suture and staples, and Dr. Cantores immediately moved on to the ankle. The patient was still awake, just tranquilized will some kind of sedative, he kept falling in and out of sleep snoring loudly.
A similar repair to Dr. Cantores’ trochanteric fracture repair. The long nail is hammered in first, and the smaller, horizontal nail is inserted afterward.
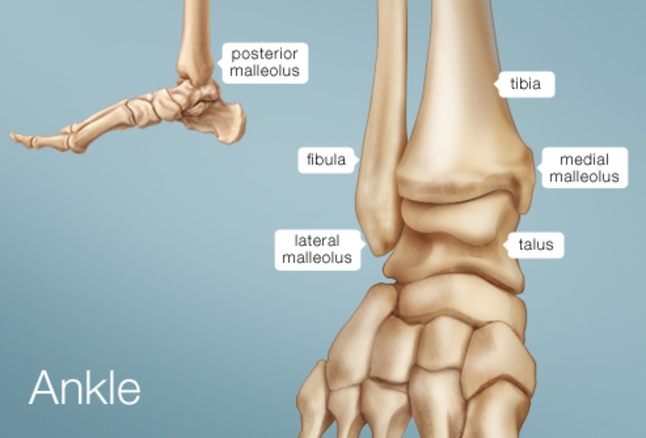
The ankle was a mess. There was both fibular and
tibular fractures on either side. The fibular fracture was horizontal so that
the tip of the fibula was free-floating. However, the tibular fracture was
vertical, right on the medial edge of the bone, as if someone took a hammer and
chipped off just the edge of the bone. He screwed a plate on to the fibula, but
for the tibia he had to insert another screw.
A little ankle anatomy. The tip of the fibula was broken right off, and the medial malleolus was broken off of the tibia.
It was another incredible day in the OR! I’ll be sure
to update you on the rest of the week. Also, feel free to leave a comment in
the comments section if you have any questions! Hasta luego!
Left to right: De’Ryonne, Dr. Nacho, Diego, and me.
The first day of my new assignment: orthopedic surgery
and traumatology. This time my partner was De’Ryonne, and we hurried over to
the first-floor meeting room for the daily report on consultations. The first
thing I noticed was that most of the physicians in the room were men and most
of them only spoke Spanish. The head of the orthopedics department, a cheerful
man in his 60s with glasses, welcomed us into the room and announced that we were
American students learning from the best surgeons in the hospital.
The orthopedic surgeons start every day with an hour of
socializing in the staff cafetería. We were told that we would follow Dr. Nacho,
a tall funny bald man and Diego, a young dark-haired resident.
Our first surgery was what Dr. Nacho called a “Hutchinson’s Fracture”, a radial fracture of the left wrist. He told us that because of the way the patient fell, he would also need to repair the ligament on the dorsal side of the wrist. In a serious ligament tear, he would remove the palmaris longus (a vestigial structure that 14% of the population does not have) from the forearm and substitute it for the torn ligament. He would then put wires between the lunate and scaphoid bones of the hand, which were separated by the fracture.
An image depicting a Hutchinson’s Fracture of the radius.
After Dr. Nacho had finished fooling around and spanking all the other orthopedic surgeons in the room, he scrubbed in and began the procedure. Dr. Nacho, Diego, and another male surgeon gathered around the drugged patient, his wrist suspended from a stand that allowed the surgeons to manipulate it into any position they wanted. The first step of the surgery was inserting an endoscope into the hand and clearing the connective tissue with a metal tool. De’Ryonne and I watched on the TV screen in anticipation. He pushed the scaphoid bone back into place and checked it with the CT scan. He then used a drill to cut into the bone to place the wire. Each time he started drilling, he yelled “radio!” and the radiologist took a picture with the CT machine so he could make sure he was drilling in the right place. The surgery didn’t seem that long, but when I checked the time it was already 1:00! We had been in surgery for about 3 hours!
Orthopedic surgery is known for the physicality of the specialty. Most of the surgeons are men because of the amount of hammering, drilling, pulling, pushing, and popping that has to be done just to realign the bones or replace the parts with prosthetics. It is easy to think of the body as a machine: when a machine breaks, you buy new parts and fix it. An orthopedic surgeon is like a mechanic, but each time the injury is different, and the mechanic has to figure out the best way to fix it whether its inserting new parts or repairing the parts already available. The other things the surgeon has to take into account for each patient is their age, mobility, and risk of a second injury.
I could already tell that orthopedic surgery was going
to be a lot of fun, and a lot of work. I can’t wait to update you on what
happened on Tuesday! Ciao!
We had an awesome weekend in Salamanca! After sleeping in our crowded hostel makeshift bed together, we all got up and got ready to go explore. The first thing we did was go to the Universidad de Salamanca, the third oldest university in all of Europe. When the university was first founded in 1138, it was only for men and you could major in one of three majors: Theology, Philosophy, or Medicine. We looked into some of the classrooms and explored the library, which had over 260,000 volumes of books.
The inner courtyard of the Universidad.Inside one of the classrooms.
After the university, we decided to explore the cathedral next door. There are two cathedrals in Salamanca: The Old Cathedral and the New Cathedral (creative, right?). We decided to explore the Old Cathedral and climb the bell tower so we could hear the bells go off at the top of the hour. The Old Cathedral was finished in the 14th century and featured a Gothic-Romanesque style roof, which we were able to climb on top of to get to the bell tower.
The Gothic-style roof of the Old Cathedral.
The Old Cathedral is the resting place of various
bishops from the 15th century, and we saw numerous tombs and altars
dedicated to saints. We hiked 200+ stairs in a very narrow spiral staircase to
get to the bells, and the view of the city was gorgeous!
One of the small prayer areas inside the Old Cathedrals, displaying intricate sculpture.The resting place of a 14th century bishop.
On Sunday, we went to the Museo de Art Deco y Art Nouveau, where I got to see works by Salvador Dali and Joan Miro. However, I was star-struck by a small gallery of lesser-known works by Pablo Picasso. My favorite was one of his numerous “woman in a chair” paintings, where he used bright yellow and pale blue to outline her shoulders and dress. Unfortunately, we weren’t allowed to take any pictures inside the museum, so there’s no proof I actually saw the paintings by Picasso. The painting was only the size of a sheet of paper, but I felt like I gazed at it for at least 20 minutes.
Lily at the top of the Cathedral, I told her to model for me.
After we finished at the museum, we went back to the train station and took the train back to Valladolid. Overall, I’d recommend Salamanca to anyone looking for some great places to explore in Spain! Ciao!
Friday was our second excursion: this time we would be learning traditional flamenco dancing from one of the most prestigious dance schools in all of Valladolid. Our flamenco teacher was a professional flamenco dancer who taught at the school. She didn’t speak any English, but she used lots of hand motions and demonstrated the steps with her body so everyone was able to follow along.
I never realized how challenging flamenco was. Steve and I have taken salsa dancing classes together, and we caught on to the steps very quickly. However, flamenco is not a partner dance, and a great majority of the movement is in the stomping of the feet. It is definitely the type of dance you need to wear heels for. She also taught us words that are specific to flamenco dancing and don’t actually translate into English. Tacon meant to tap your heel to the ground and golpe meant to stomp your whole foot. It was like learning how to dance and learning a new language all at once.
All of us with our flamenco teacher, doing a flamenco pose.
We went out to lunch after flamenco dancing, and then relaxed until 5:00 when we jumped on a train to go to Salamanca for the weekend. Salamanca is a city that is about an hour from Valladolid that is known for being home to the third oldest university in all of Europe: Universidad de Salamanca. I fell asleep on the train (like I always do) and Lily, Ethan, and Kyle had some fun taking pictures with me while I was asleep.
Me sleeping.Ethan, Lily, me, and Kyle on the train. I was out for sure.
We finally arrived in Salamanca, and we split two rooms in a cheap hotel among 10 people (5 per room). We had to sleep sideways across two twin beds pushed together but it worked out fine, and that evening we went out to a nice dinner at an Italian restaurant that specialized in pizzas.
A building in Salamanca.A mural I first noticed when we arrived in Salamanca.
I’m sorry I’ve been slacking about updating the blog everyday, but I’m catching up slowly but surely! Keep posted. Ciao!
Thursday was our last day shadowing in the urology department. I thought back to how I had felt about urology before shadowing in the department, and I realized that my mind had changed drastically. I no longer think that becoming a “Pee-Doctor” is lame, or that spending 8 years specializing in the prostate was strange. Never judge a book (or a medical specialty) by its cover.
Today we were watching a nephrectomy (removal of the kidney) for a patient who had a LARGE tumor (5-6cm) on their left kidney. Unlike the partial nephrectomy we saw on day 2, the surgeon clamped the artery first and then the vein. This way, the kidney would be mostly drained of blood before it was taken out of the body of the patient.
Saman and I underestimated how exhausted we were from the rest of the week, and by the time we were in the OR we were falling asleep standing up. The surgery was about 4 hours and we took observations and asked questions about the procedure, which was mostly done by our resident friend Sarah.
After urology, I had to go to English tutoring with Dr. Moya. I found her in the ER, and she was overwhelmed with an incredible amount of new patients. “Let me show you an interesting case” she said, leading me into a patient-room. There was a woman with the worst jaundice I had ever seen: her skin was a dark yellow-brown color, and her eyes were bright amber where they should have been white. Dr. Moya told me that this patient had not had any symptoms other than abdominal pain and the jaundice, but she suspected pancreatic cancer: a cancer that is very difficult to diagnose. I was amazed at Dr. Moya’s intelligence and her way of talking to patients in a compassionate, yet straightforward way.
I hope to continue to learn her secrets and understand what it is to be not only a great physician but a great person. Even without understanding all of the language, I can tell she truly cares for her patients and they love and appreciate her even more.
Today was wild. Not only did Saman and I shadow in the greatest department in the entire hospital yet again (urology), but we saw 4 surgeries in a row!
Saman and I on a coffee break.
The first surgery we say was a kidney stone removal. We changed into our scrubs and met our surgeon we were shadowing in the operating room. The patient was already knocked out in supine position on the table, and the residents were painting the abdomen with povidone iodine (an antiseptic that appears orange).
We never actually caught our surgeon’s name, and so we decided to refer to him as “Super-Surgeon” after what we saw today (I’ll go into the details). Super-Surgeon told us that there are 3 ways to remove kidney stones in a patient: shock wave lithotripsy, laparoscopy, and something he referred to as “BNL”. BNL was invented in 1994 in Spain, and would be the procedure that we would be using today where the patient is put in supine and both a laparoscope and a catheter would be inserted so that all the stones could be retrieved (something called the “retrograde laparoscopic approach”). He told us that in the U.S., this procedure is performed in prone position but this is not as good because it is harder for the anesthesiologist to reach the patient’s airways. Contrast was inserted into the catheter and the physicians used a CT scan to see where the 3 cm right kidney stone was. The doctors used an endoscope and a tiny laser to break up the stone. It looked like a video game: the surgeon found the stone which looked like an asteroid and then aimed and shot at it until it broke into tiny pieces.
Saman and I with our favorite doctor whom we call “Super Surgeon”.
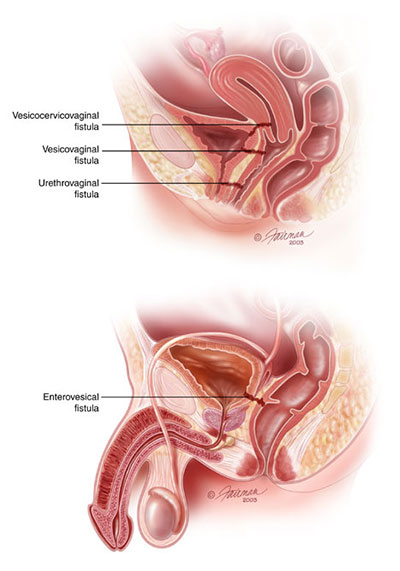
As our first surgery came to a close, Super-Surgeon told us to peek into OR 5 to see what they were up to in there. We walked in. It was dark, and everyone was huddled around the TV above the operating table wearing sunglasses. The first thing I thought was, why are they wearing sunglasses? Sarah the resident walked up to us and handed us sunglasses, and as soon as I put them on I realized why everyone was wearing them. They were 3D glasses and all the surgeons were observing the surgery in 3D! After the robot surgery on the first day, I thought the urology department couldn’t get any more advanced, but I was proven wrong. They were repairing a fistula (hole) that had developed between the large intestine and the bladder.
A representation of different types of fistulas in male and female patients.
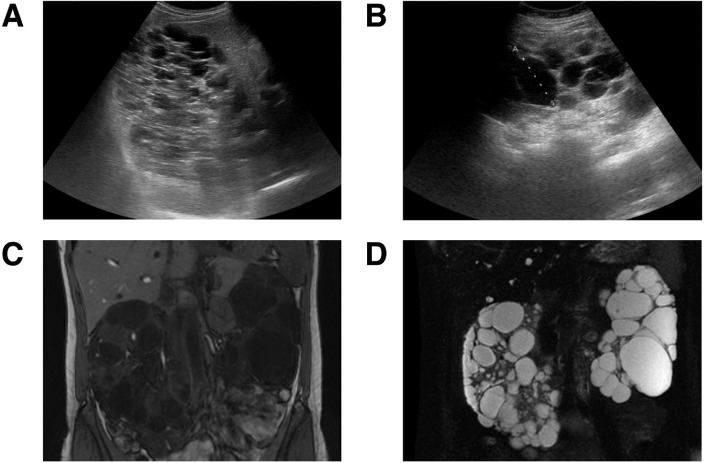
The third surgery was a patient that needed kidney stone removal from their transplanted kidney. The patient was relatively young with a genetic form of renal polycystosis: a disease where the kidneys develop non-cancerous cysts that cause the kidneys to lose function overtime. We were able to look at the patient’s kidneys on the CT scan: they were incredibly swollen and bumpy, I had never seen kidneys that looked so strange before! Super-Surgeon explained that a kidney stone removal from a transplanted kidney is more difficult than from a natural kidney because it is harder to find the entrance of the ureter into the bladder, and sometimes the ureter is narrowed. When the ureter is narrowed, there is a higher probability of infection, and in a patient with a compromised immune system this can be very dangerous. When Super-Surgeon entered the bladder and viewed the ureter through the endoscope, he realized it was too narrow to begin the stone removal process. He placed a stent in the ureter and informed us that he would check it in approximately 2 weeks and complete the full surgery.
I found this picture on the internet: a ultrasound and CT scan depicting renal polycystosis. (sciencedirect.com)
Finally, we made it to the last and final surgery of the day. It was another kidney stone removal, but this patient had a congenital (from birth) disorder called medullary sponge kidney. In medullary sponge kidney, the collecting tubules are dilated, promoting the development of kidney stones. However, the stones are not able to leave the kidneys because they are stuck behind a mucous membrane. Super-Surgeon told us that the main goal of this surgery would be to break the mucus membrane, allowing the kidneys to “give birth” (his words, not mine) to the stones. He would pulverize the bigger stones into dust so that the patient could easily pass the stones by themselves.
By the time we finished observing the last surgery, we were exhausted. We got lunch and headed back to the dorms, and later that night we all went out for dinner together and got a nice group picture in front of the Iglesia de San Pablo, seen below:
I know this post is a little late, but I will be sure to catch up and continue to update you all on the crazy things (in and out of the hospital) I see in Spain! Ciao!
Today was the second day at the hospital, and it was just as amazing as the first. Saman and I arrived a little early for our rotation, so we found the hospital library and began to read up on the surgery that we would be observing today: a partial nephrectomy.
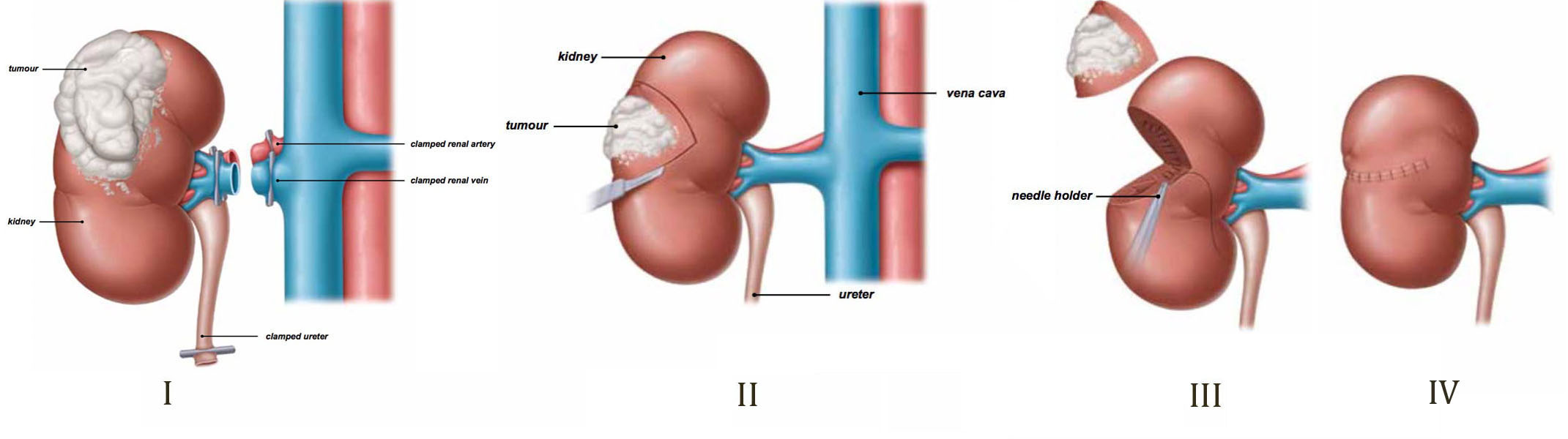
In a partial nephrectomy, the surgeon removes a tumor that has formed on the kidney, without removing the kidney. This surgery was performed using a laparoscope. Laparoscopy came before the Da Vinci robot, and consists of the surgeon making small incisions to insert a camera and perform the surgery inside the patient. This patient had a golf-ball sized tumor on the superior portion of the left kidney.
The surgeon first exposed and clamped the renal vein, then began to expose the kidney. The trickiest part about this surgery is that as soon as the renal artery is clamped, the tumor has to be removed within 40 minutes or the kidney will stroke. The tumor looked like a ball-shaped trunk covered in fat, kinda like a strange-shaped cauliflower. Once the tumor was exposed, the surgeon clamped the renal artery. I looked at the clock: 11:51.
A diagram of a partial nephrectomy.
Saman and I watched in anticipation as the surgeon began cauterizing the tissue around the tumor, loosening it from the kidney surface. The camera angle was amazing, I could clearly see the spleen snuggled up against the lateral abdominal wall, and in the background the diaphragm slowly rose and fell like a red sunset in an alien movie. The tumor was finally free! However, now the kidney was cut open, and the surgeon began suturing the hole created by the tumor. By the time he was done suturing, I looked at the clock: 12:15! He performed the whole procedure in only 24 minutes! Amazing!
The residents finished closing up the patient and asked us if we had any specific questions. After the surgery, we changed back into our lab coats and went to the cafeteria to eat and tell the other fellows of the things we saw.
Later that night we went out for dinner at a Chinese resturant and went shopping a little bit. Liliana, Irene, De’Ryonne and I walked together and chatted, we had a great time exploring the city as the sun went down. I can’t wait for another great day at the hospital tomorrow! Ciao!