

On Tuesday, De’Ryonne and I were with a different surgeon, a man named Dr. Jose Cantores. He was a middle-aged man with dark hair who spoke English very well. Our first surgery was a man in his 30s with a right knee fracture and a medial ligament tear. When I asked Dr. Cantores how this man got his injuries, all he said was “he jumped off of something”.
Dr. Cantores waited about 10 minutes for the epidural to kick in and then grabbed the cauterizing knife and went straight for the lateral knee. He opened the joint capsule and cut through the lateral meniscus, where he found the broken fragment from the fibula. Using the CT scan to position the drill, he inserted a plate and attached it to the bone with pins. There was a little extra space between the broken fragment and the fibula, which he filled with crumbles of bone donated from a human cadaver. When I asked about it, Dr. Cantores told us that the patient’s body would eventually replace the donated bone crumbles, but it would work as a structural substitute until the bone started to grow back. After the plate was positioned, he removed all the pins and placed 6 screws in instead to stabilize. He sutured the muscle back into place, and stapled the skin. Dr. Cantores told us that the patient would recover in about 2 weeks, but would need to be non-weight bearing during recovery.
We quickly moved on to our second surgery: a trauma case where a man had a hip fracture on his left leg and a broken ankle on his right leg. The patient was pretty beaten up from head to toe, it looked as if he had fallen down an extensive staircase and scraped and bruised his head, face, chest, knees, and feet. His ankle was purple and swollen, and after they removed his clothes you could tell that his hip was slightly swollen as well. The nurses hung up a giant sheet of clear plastic in front of the surgeon and the hip so that the patient was on one side, and the surgeon was on the other. There was a tiny hole where Dr. Cantores could access the hip, but I had never seen something like this before. Dr. Cantores called it the “Vertical System”, a way to keep things completely sterile but also allow the surgeon to view the patient. He told us: “Prevention is the only way to avoid infection”, and that the Rio Hortega Hospital prides itself on being completely microbe-free.
The hip fracture was located right under the trochanter of the femur, so Dr. Cantores hammered in a large nail right through the fracture and into the center of the femur bone. A screw was placed horizontally towards the head of the femur to hold the nail in place. An additional smaller pin was placed further down the femur to stabilize the nail. The wounds were closed with suture and staples, and Dr. Cantores immediately moved on to the ankle. The patient was still awake, just tranquilized will some kind of sedative, he kept falling in and out of sleep snoring loudly.

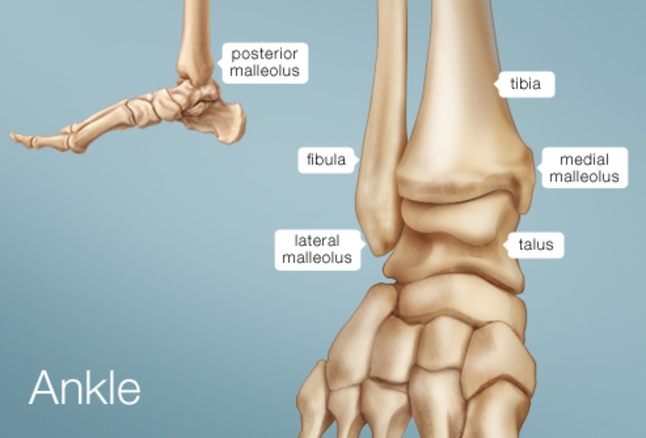
The ankle was a mess. There was both fibular and tibular fractures on either side. The fibular fracture was horizontal so that the tip of the fibula was free-floating. However, the tibular fracture was vertical, right on the medial edge of the bone, as if someone took a hammer and chipped off just the edge of the bone. He screwed a plate on to the fibula, but for the tibia he had to insert another screw.
It was another incredible day in the OR! I’ll be sure to update you on the rest of the week. Also, feel free to leave a comment in the comments section if you have any questions! Hasta luego!
